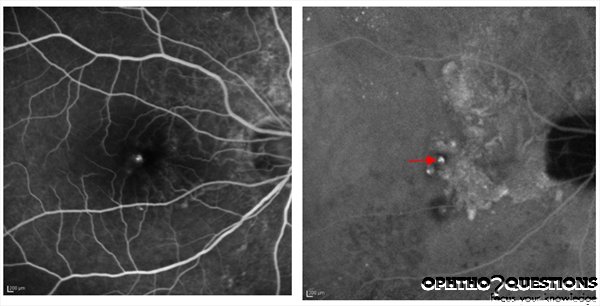
A 73-year-old man complains of sudden painless vision loss in the right
eye. The fluorescein angiogram (FA) and indocyanine green angiogram
(ICG) (late phase) are shown. Which of the following is TRUE regarding
this patient's disease?
Retina and Vitreous
Acquired Diseases Affecting the Macula
No
U
C
Polypoidal choroidal vasculopathy (PCV) was originally described by Yannuzzi et al in 1982 as a distinct form of choroidal neovascularization with a predilection for the peripapillary area. It is characterized by dilated choroidal vascular channels terminating in "polyps" leading to serous and hemorrhagic detachments of the retina and RPE. Another key feature is that there is either minimal or no cystic change of the overlying retina even if the subretinal hemorrhage is severe.
PCV is best diagnosed through ICG angiography. In the photos above, a
polyp is highlighted as a hyperfluorescent spot on ICG (arrow). The
branching vascular network is seen nasal to the polyp.
Although PCV is thought to occur more commonly in pigmented races, with
increased use of ICG, it is being discovered that PCV is underdiagnosed
in nonpigmented races. The EVEREST trial1
demonstrated an increased rate of anatomical closure of polyps in PDT +
ranibizumab as compared with ranibizumab monotherapy or PDT alone.
1Koh A et al. EVEREST STUDY: Efficacy and Safety of
Verteporfin Photodynamic Therapy in Combination with Ranibizumab or
Alone Versus Ranibizumab Monotherapy in Patients with Symptomatic
Macular Polypoidal Choroidal Vasculopathy. Retina. 2012 Mar 21.
Heads up! You can use keyboard for test navigation: press → for Next,
← for Previous, M for Mark/Unmark, P for Pause,
R for Review, A,B,C,... or 1,2,3,... to select answer.